Panpharmacon's Polypharmacy
Panpharmacon's Polypharmacy
Be wary of salience and efficacy conflation

I was recently confronted with the fact that I’m a huge outlier. While this might apply across a few distributions, in this instance it was while reading Troof’s comparatively large (n=1981) survey of nootropics and their attendant reported efficacies. He did it in a clever way that involved an ostensible recommender system that first required input and rating of all previously used psychotropics (and a few behavioral interventions + performance enhancers that might not strictly qualify as ‘nootropics’, as nebulous as that term is).
I say I’m an outlier in that I’ve tried basically all of the compounds listed in the final reported analysis (see the chart below). In fact I’ve taken way more. E.g., I tried high-dose semaglutide at 11% body fat out of essentially a pathologic curiosity, and I’ve insufflated synthetic, bio-equivalent Orexin-A. I use the qualifying ‘basically’ because there are a few in specific classes like the racetams for which I haven’t tried all of the species, but these groups also have largely the same mechanisms of action. I also haven’t used St. John’s Wort as it induces several CYP enzymes and can foment myriad negative downstream effects on the metabolism of other drugs and supplements. I recommend taking a serious look at this supplement on a reputable CDSS database like Dynamed or UpToDate. Examine.com is also an indispensable resource, but more on that in future post.
Here’s the chart:
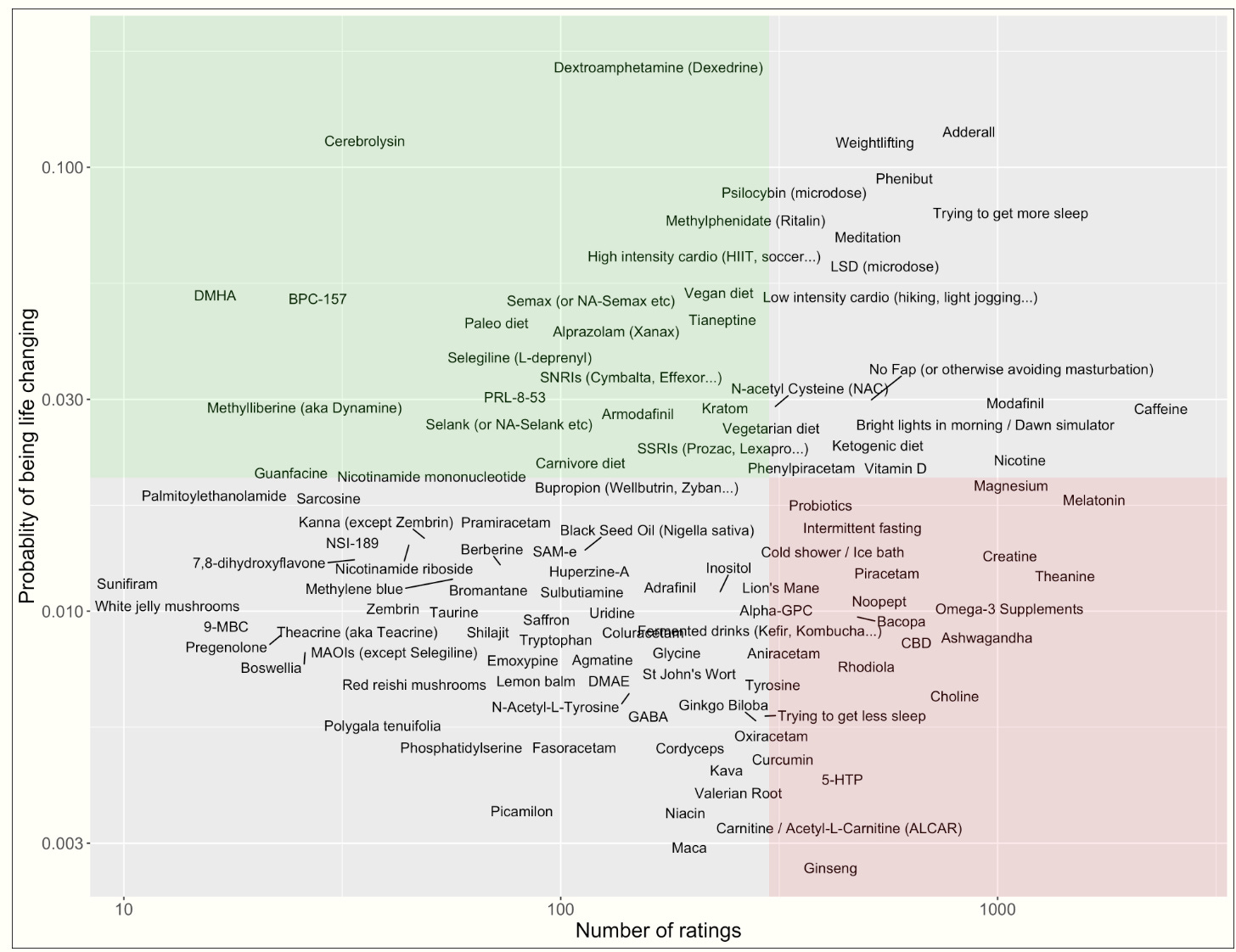
Source link
Certainly some caveats apply:
Selection bias is playing a role here. The type of person to seek out this survey and complete the rather tortuous recommender system is very interested in cognitive augmentation and/or has a reason for trying some of the more serious drugs here.
Some of these compounds have varying levels of legality in different jurisdictions, thus it could take a relatively sophisticated user to obtain prescription stimulants or Russian-sourced peptides like BPC-157 and Cerebrolysin.
The chart is on a log scale, so ratings and # of reported users are more spread out than they may appear.
A few compounds are left out of this analysis that I feel warrant review.
Now I understand that it may come off as a bit outré that a blog premised on promoting parsimony in supplementing psychotropics has tried the 100+ psychotropics list above. It definitely is. But what I can say is that I took each compound in relative isolation usually with some control comparison and washout period like the good little scientist I am. I also have done so over the span of ~10 years, so it may not be quite as outlandish as it first seems.
Another feature of my personality is strict monomania. If I’m going to do or probe something, I do it. E.g., I spent a full 2 years in continuous ketosis (wouldn’t recommend, but that’s also for another post) as measured by CGM, breath acetone, and serum beta-hydroxybutyrate concentrations. In a way it’s a healthy sublimation technique for an addictive personality type.
The Best Nootropics
So what is driving the y-axis rating differences among the experimented compounds? For one, ‘probability of being life changing’ is a weird benchmark. But the most salient factor to me is salience. The highest rated compounds are by far the most psychoactively appreciable (e.g., the amphetamine drugs and the psychedelics). This is fine for quick fluid IQ bumps (and maybe some long term neuroplasticity changes with chronic dosing of psychostimulants), but it heavily discounts the returns to long-term, assiduous implementation of exercise, sleep hygiene, cognitive exercise, omega-3 supplementation, and perhaps some intermittent fasting (there is some evidence that fasted states precipitate catecholamine and acetylcholine release in certain brain regions).
Maybe this is more a commentary on the primacy of behavioral interventions, but there is a premium on instant gratification in these rankings that I don’t like. Indeed on the whole nootropics users seem to be in search of Limitless-like panpharmacon that is likely non-existent. Though the homeostatic theory of drug tolerance isn’t a 100% perfect law, compensatory brain changes do occur and returns to use of psychostimulants will invariably diminish with use (and only return on long timescales). Forbearance is one of the greatest virtues with respect to cognitive enhancers, and you’re almost always better off practicing your Anki cards and exercising as opposed to sniffing Semax for the ephemeral BDNF boost.
With all that in mind, here’s a perfunctory overview of what I believe are the best, most sustainable exogenous cognitive enhancers:
Re-esterified DHA/EPA (DHA makes up a huge proportion of fatty acid concentrations in the brain & it’s evolutionarily consistent that Omega-3s were a much higher proportion of the Homo sapiens diet for much of our ancestral past.
The ‘Lindy’ Ones: Nicotine & Caffeine. They actually have similar addiction and tolerance potentials, with a major difference being pharmacokinetic: nicotine has a duration of action of ~1 hour and caffeine of ~5 hours (though this depends on individual differences). The notable difference is nicotine’s short half-life foments chronic re-dosing so caution is warranted. Further, the speed of nicotine’s delivery mechanism to the brain is directly proportional to it’s addictive potential: inhalation, buccal administration, and ingestion, in descending order. And further carcinogenic risks are present for certain delivery types (mainly combustion, but see Examine.com for more fulsome details). I like nicotine gum.
Eating enough protein to supply the precursor amino acid substrate for many neurotransmitters and neurohormones.
On the converse, I recommend you don’t take:
Any fat soluble vitamin without blood testing and a specific reason for doing so. These can build up in the body and foment serious problems.
Almost any GABAergic (i.e., Xanax, but also Kava Kava, Ashwagandha, Alcohol, maybe Theanine, Taurine and Beta-Alanine in isolation, and many others). Even glycine, though not a direct GABA(a) agonist, acts on a similar type of receptor and is not entirely as benign as many believe. Only two classes of drugs will kill you in withdrawal: Benzodiazepines/Barbiturates + Alcohol. These all modify GABA(a) receptors as some flavor of agonist or positive allosteric modulator (or both), both synaptic and extrasynaptic, and will alter your brain’s inhibitory: excitatory ratio unfavorably. Phenibut and Balcofen (two GABA(b) receptor agonists) are a bit different, but extreme caution is warranted.
Magnesium, except in very low doses. This will engender some controversy, but hypermagnesia risk is higher than most realize, it’s a more potent anti-dopaminergic than many realize, it can function as a quasi-soporific agent, and NMDA quasi-antagonism will attenuate learning ability. I will write more on this eventually, but Gwern has a good write-up on his self-experimentation with magnesium.
I think there may be some bathos in recommending the time-worn, conventional nootropics, but they are popular and instrumental for a reason. I further think that there is a beneficial use-case for some of the more novel peptides like Sermorelin and Cerebrolysin. I will do a write-up on my use of the latter in the future, but for now I’ll leave it at that.